Structure Literacy Teacher (SLT) is a fairly new label, developed by the International Dyslexia Association (IDA), to describe the most effective form of instruction for students identified dyslexic. This type of instruction is also effective for English Second Language (ESL) learners and for other students at-risk for literacy acquisition (Baker et al., 2014; Gersten et al., 2009). Structured literacy instruction should include following instructional principles:
- systematic instruction, taught in logical order—builds upon prior knowledge
- students should learn the foundational or prerequisite skills of the current lesson
- explicit instruction, direct—clearly explained and teacher modeled
- scaffolded instruction to match student abilities, providing exact temporary support
- interactive discussions about the “new” task
- multiple opportunities to practice the new task or skill
- monitoring of student achievement through observation, interaction, and formal assessment
Structured literacy instruction includes six pillars or parts of literacy development—oral and written. Structured literacy instruction should begin with Pillar 1, as each is dependent on the previous pillar(s).
Pillar 1 is phonology, the study of spoken sounds (phonemes)—rules of how sounds are encoded, such as why these sounds follow this pattern to form this sound(s). Individuals should have phoneme awareness skills before learning how to read. This is the ability to hear, identify, and manipulated individuals sounds in spoken words. Phoneme awareness is part of phonological awareness. Phonological awareness is the ability to process and manipulate letter sounds, rhyming words, and segmenting of sounds within words. The study of phonology usually increases student ability to spell, pronounce, and comprehend written words.
Pillar 2 is sound-symbol correspondences or the relationship(s) between phoneme(s) and grapheme(s). This may be referred to as phonics instruction that teaches predictable or the constant rules of sound-symbol correspondences to produce written language. At this stage students learn one-on-one correspondence, for example the written letter B represents this phoneme or sound. It is important to note that some letters are represented by more than one sound, depending on the origin and spelling of the word. Students begin decoding and encoding words as they begin to learn the sound-symbol correspondences. Student knowledge of the phoneme(s) and grapheme(s) relationships usually increases student ability to read, comprehend, and spell written language.
Pillar 3 is syllable knowledge, the understanding of the different types of syllables. Syllable knowledge increases the accuracy of language pronunciation and comprehension. Syllable knowledge also increases student decoding and encoding skills. The English language has six major types of syllables that are described in the following chart.
|
Type of syllable
|
Example
|
|
CVC
|
cat, log, bit, set, cut
|
|
Final e
|
kite, bone, bake, cute
|
|
Open
|
me, sky, be/gan, mu/sic, fe/ver
|
|
Vowel Diagraph
|
oi-soil, oil; ee-sleep, keep; ea-beat, leak; oa-boat, road; oo-zoom, smooth
|
|
r-controlled
|
ar-car, start; ir-girl, swirl; er-her, flower; ur-fur, burn; or-fork, corn
|
|
Constant-le
|
marble, puddle, bugle, maple, little
|
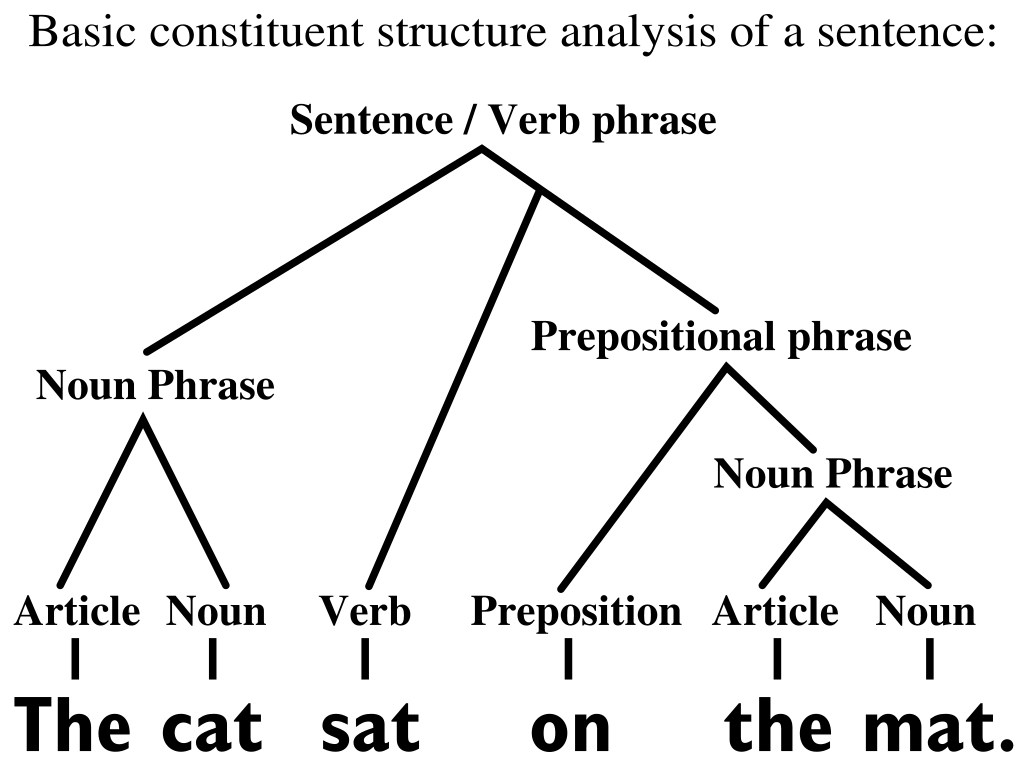
Pillar 5 of structured literacy instruction is syntax or the study of sentence structure. The principles that dictate the sequence and function of words in a sentence. These principles are also referred to as the mechanics, grammar, and variation of a sentence. Pillar 4 is morphology that is the study of the smallest units of meaning or morphemes. Morphology focuses on how parts of meaning fit together to form words and new meaning. Word analysis helps students to learn the meaning(s) of morphemes and how the word parts conclude its meaning. Word analysis also increases student background knowledge, which increases student ability to comprehend written passages.
The more common parts of a sentence.
|
Parts of a sentence
|
Definition
|
Examples
|
|
Verb
|
describes the action
|
bark, ran, call, like
|
|
Adverb
|
modifies a verb, helps to clarify or further define a verb
|
warmly, quiet, loudly, today, outside
|
|
Noun
|
person, place or thing
|
house, dog, car, book
|
|
Adjective
|
modifies a noun, adjusts the meaning or further defines the noun to clarify meaning
|
beautiful, dark, old
|
|
Article
|
determiners, modifies and precedes a noun
|
a, an, the
|
|
Preposition
|
usually precedes a noun and in relation to another word in the clause
|
at, in, on, with, for, about, of, after
|
|
Conjunction
|
connecting words, they connect clauses and sentences
|
and, but, if
|
Pillar 6 of structured literacy is semantics or study of the meaning of words, symbols, and units of words. A person’s lexicon stores the meaning of words, symbols, and units of words—vocabulary. People begin to develop their lexicon at birth. Individuals attach meaning to tones of sound. These meanings are adjusted as individuals are introduced to new tones or meanings. Individuals transfer the meaning of tones (voice) to symbols (print) as they learn how to read and write. To better understand words and groups of words teachers often use concept maps to examine the definition of a word. Students identify the related synonyms and antonyms of the word. Students often identify or attach pictures to a word or groups of words. Semantics assist in attaching inferred meaning to written and oral verbiage. Semantics can include morphology.
You can find details about becoming a certified Structured Literacy Teacher on the IDA website.
References
Baker, S., Lesaux, N., Jayanthi, M., Dimino, J., Proctor, C.P., Morris, J., Gersten, R., Haymond, K., Kieffer, M.J., Linan-Thompson, S., & Newman-Gonchar, R. (2014). Teaching academic content and literacy to English learners in elementary and middle school (NCEE 2014-4012). Washington, DC: National Center for Education Evaluation and Regional Assistance (NCEE), Institute of education Sciences, U.S. Department of Education. Retrieved from http://ies.ed.gov/ncee/wwc/publications_reviews.aspx.
Gersten, R., Compton, D., Connor, C.M., Dimino, J., Santoro, L., Linan-Thompson, S., & Tilly, W.D. (2009). Assisting students struggling with reading: Response to intervention and multi-tier intervention for reading in the primary grades, a practice guide (NCEE 2009-4045). Washington, DC: National Center for Education Evaluation and Regional Assistance (NCEE), Institute of education Sciences, U.S. Department of Education. Retrieved from http://ies.ed.gov/ncee/wwc/publications/practiceguides/.